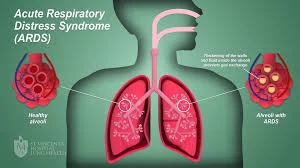
Glenohumeral joint (GHJ) osteoarthritis (OA), or shoulder arthritis, is a painful, progressive and debilitating condition that impairs quality of life. The symptoms of shoulder osteoarthritis typically develop slowly and worsen over time. The most common symptom is pain that is worse with activity and improves with rest. Other symptoms may include stiffness, weakness, and crackling or grating sensations when the shoulder is moved.
Shoulder osteoarthritis is caused by the damage and reduction of the cartilage that cushions the ends of the bones in the shoulder joint. This can be due to age-related wear and tear, injury, or repetitive use of the shoulder. This condition has traditionally been managed with total shoulder arthroplasty, a major operation that carries significant risks.
Therefore, initial management of shoulder arthritis aims to provide symptom control in order to delay or prevent the need for joint replacement. Nonoperative management modalities such as physical therapy, pain-control medications, and intra-articular injections are initially recommended. Of these treatments, corticosteroid injections are the most commonly used because they have been shown to provide short-lived pain relief.
Intra-articular hyaluronic acid injections also offer a clinically significant improvement in pain and function for up to 6 months after injection, but there is limited information on their use specifically for GHJ OA. Recently, bone marrow aspirate concentrate (BMAC) and bone marrow aspirate (BMA) injections have recently become available as treatment options for OA symptoms and may be more effective than other injectables in providing longer-lasting relief from pain.
BMA/BMAC use involves injecting a patient’s own stem cells into the affected joint, which can potentially reduce inflammation and induce the regeneration of cartilage tissue over time. These treatments have been found to improve joint mobility as well as reduce pain levels when compared to corticosteroid injections. However, further research is needed to validate its long-term benefits.
A study, Injection of Bone Marrow Aspirate for Glenohumeral Joint Osteoarthritis: A Pilot Randomized Control Trial, looked into how patients can utilize stem cells to improve shoulder osteoarthritis outcomes.
Results of the Study
The goal of this study was to compare the efficacy of stem cell therapy to cortisone injection for the treatment of shoulder arthritis. The researchers recruited 22 patients, for a total of 25 shoulders, who were suffering from shoulder arthritis. The patients were split into two randomized groups.
Twelve shoulders received cortisone shots, and 13 shoulders received BMA. The BMA group had BMA taken from their spinal cord and then was processed and given to patients via intra-articular injection. The hope was that the BMA injections, rich in stem cells, would improve patient outcomes.
The researchers evaluated patients using Western Ontario Osteoarthritis of the Shoulder (WOOS), QuickDash, EQ-5D-5L, and visual analog scale (VAS) for pain. Unfortunately, the study was cut short due to changes in Health Canada regulations. Some patients who were enrolled in the study were unable to receive the treatment. However, the researchers were able to follow the patients who were treated for 12 months after they received their treatment. There were no significant adverse events from the BMA treatment.
The results of the study were promising for patients suffering from shoulder arthritis. Mean WOOS scores improved from 1082 to 684 12 months after receiving the stem cell treatment. Meanwhile, mean WOOS scores in the cortisone group only improved from 1088.9 to 1002.7 after 12 months.
QuickDASH scores also saw similar improvements. Mean QuickDASH scores improved from 42.5 to 25.5 in the BMA group after 12 months, while the cortisone group only improved from 39.4 to 37.1. VAS scores saw some improvement, going from a mean score of 4.3 to 3.0. Additionally, EQ5D-5L pain scores improved from 3 to 2 after 12 months in the stem cell therapy group.
The study found that after 12 months, BMA injections were associated with significantly greater improvements in QuickDASH and EQ-5D-5L pain and health scores than Cortisone injections. On the WOOS primary outcome measure, there was no significant difference between the two treatments. However, the study was underpowered due to early termination, which limits its conclusions, and further research is needed to confirm these findings.
BMA injection therapy has been shown to have long-term effects on tissue healing, nerve regeneration, and reducing inflammation. On the other hand, cortisone injections are primarily used for pain relief but do not have any long-term benefits on tissue health or healing. Therefore, it is possible that BMA injection therapy may be more effective in the long run in terms of restoring function and improving quality of life when compared to cortisone injections.
Learn more about stem cell therapy at BioXcellerator.com.